
More than 1 in 10 people believe they have a drug allergy. But here’s the surprising truth: most of them don’t. A label like "penicillin allergy" sticks for life-even if it was based on a mild rash from childhood, or a fever that had nothing to do with the medicine. And that mislabeling isn’t just inconvenient. It can be dangerous.
Penicillin: The Most Misunderstood Drug Allergy
Penicillin and its relatives-like amoxicillin-are the most common drugs blamed for allergic reactions. About 10% of Americans say they’re allergic to penicillin. But when tested properly, over 90% of those people aren’t allergic at all. Why? Because many reactions aren’t allergies. A stomachache, a rash that clears up on its own, or even a viral infection mistaken for a drug reaction gets labeled as "allergy" and never questioned again.
The real danger? When someone is labeled allergic to penicillin, doctors avoid it-even when it’s the best, safest, cheapest option. Instead, they use broader-spectrum antibiotics like vancomycin or fluoroquinolones. These drugs are more expensive, less effective against common infections, and increase the risk of dangerous superbugs like C. diff. Studies show patients with a penicillin allergy label stay in the hospital half a day longer and pay over $1,000 more per admission.
The good news? Testing is simple and accurate. Skin testing with penicillin derivatives, followed by a small oral dose of amoxicillin, is 97-99% reliable. In Australia, more hospitals are starting these tests. If you were told you’re allergic to penicillin as a kid, it’s worth getting retested. Most people outgrow it after 10 years without exposure.
Other Antibiotics That Trigger Reactions
Penicillin isn’t the only antibiotic that causes trouble. Sulfonamide antibiotics-like Bactrim (trimethoprim-sulfamethoxazole)-cause reactions in about 3% of the general population. But for people living with HIV, that number jumps to 60%. These reactions often show up as a rash, fever, or liver problems. They’re not always IgE-mediated, so skin tests don’t always work. The key is recognizing the pattern: if a rash appears 7-14 days after starting the drug, it’s likely a delayed hypersensitivity reaction.
Cephalosporins-like cephalexin or ceftriaxone-are often avoided in people with penicillin allergies. But the cross-reactivity risk is now known to be only 1-3%, not the old 10% myth. If you’ve had a mild reaction to penicillin, you’re likely fine with most cephalosporins. Your doctor should check the specific class and your history before ruling them out.
NSAIDs: More Than Just Stomach Upset
NSAIDs like ibuprofen, naproxen, and aspirin are the second most common trigger for drug hypersensitivity. But their reactions are different. Most aren’t IgE-mediated allergies. Instead, they interfere with the body’s natural inflammation pathways, causing symptoms like wheezing, nasal congestion, or hives-especially in people with asthma or nasal polyps.
Aspirin-exacerbated respiratory disease affects 7% of adults with asthma and 14% with nasal polyps. These patients can’t tolerate any NSAID, not just aspirin. They need to avoid all non-selective NSAIDs and often require steroid treatments to manage their symptoms. Even a single dose of ibuprofen can trigger a severe asthma attack in these individuals.
Here’s a key point: if you’ve had a reaction to one NSAID, you might still be able to take another. Celecoxib (Celebrex), for example, is often tolerated because it doesn’t affect the same enzyme pathway. But you need to be tested under medical supervision before trying.
Anticonvulsants and the Hidden Genetic Risk
Some drug reactions aren’t just allergic-they’re life-threatening. Carbamazepine (Tegretol), used for epilepsy and nerve pain, can trigger Stevens-Johnson syndrome (SJS) or toxic epidermal necrolysis (TEN). These are rare but deadly skin conditions where the top layer of skin peels off, like a severe burn.
The risk isn’t random. People with the HLA-B*1502 gene variant have a 100-fold higher chance of developing SJS/TEN when taking carbamazepine. This variant is common in Southeast Asian populations-up to 15% in Thai, Malaysian, and Chinese groups-but rare in Europeans or Africans. Because of this, the FDA now recommends genetic testing before prescribing carbamazepine to anyone with Asian ancestry. In Taiwan, where screening became routine, SJS/TEN cases dropped by 90%.
Lamotrigine (Lamictal) is another anticonvulsant linked to rash. About 5-10% of users develop a rash, and in 1 out of every 1,000 patients, it can turn serious. The rash usually appears within the first 8 weeks. If it spreads or is accompanied by fever or blisters, stop the drug immediately and get help.
Chemotherapy and Biologics: When the Cure Causes a Reaction
Cancer treatments are especially tricky. Drugs like paclitaxel (Taxol) cause hypersensitivity reactions in up to 41% of patients. These often happen during the first infusion-flushing, shortness of breath, low blood pressure. Most are managed with premedication: steroids, antihistamines, and slowing the infusion rate.
Monoclonal antibodies like cetuximab (Erbitux) are even more unpredictable. In Australia and the U.S., about 2% of patients have severe anaphylaxis on first exposure. Why? Some people have pre-existing IgE antibodies to a sugar molecule (alpha-gal) found in the drug, which they developed after a tick bite. It’s a rare but growing cause of drug reactions.
These reactions aren’t always avoidable. For cancer patients, the benefits outweigh the risks. But allergists now use desensitization protocols-gradually increasing doses under close monitoring-to safely give these drugs to patients who’ve had reactions before.
Radiation Dyes and the Silent Risk
Contrast dyes used in CT scans and X-rays trigger reactions in 1-3% of patients. Most are mild-itching, nausea, or a metallic taste. But 1 in 2,500 people have a severe reaction, including anaphylaxis.
Here’s something surprising: these reactions aren’t true allergies. They don’t involve IgE. Instead, the dye directly triggers mast cells to release histamine. That’s why antihistamines and steroids help-they block the body’s response, not because they’re treating an allergy.
Premedication cuts moderate-to-severe reactions from 12.7% to just 1%. If you’ve had a reaction before, you’re at higher risk. Tell your radiologist. They’ll give you a steroid and antihistamine before the scan. Newer contrast agents are safer, but you still need to be monitored.
How to Know If It’s Really an Allergy
Not every bad reaction is an allergy. Here’s how to tell:
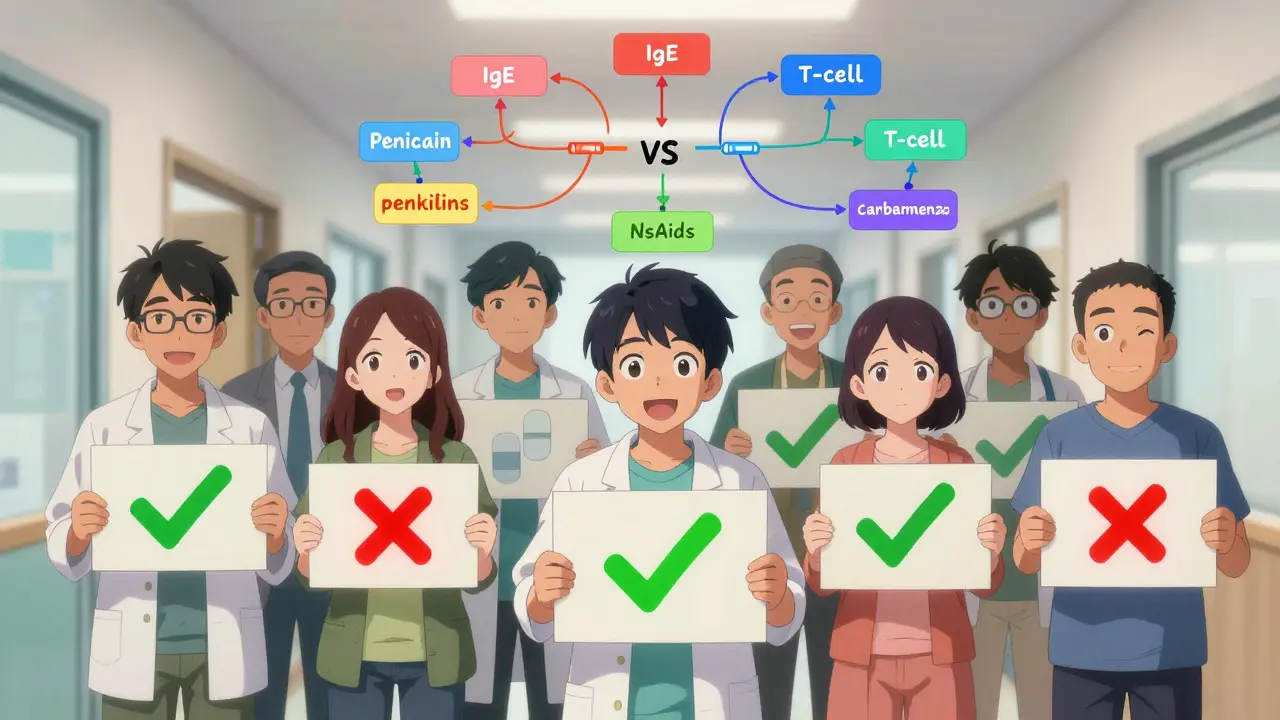
- True allergy (IgE-mediated): Happens within minutes to an hour. Symptoms: hives, swelling, wheezing, drop in blood pressure, anaphylaxis.
- Delayed reaction (T-cell mediated): Appears 24 hours to weeks later. Symptoms: rash, fever, liver inflammation, blistering skin (like SJS).
- Non-allergic reaction: Nausea, dizziness, headache, stomach upset. These are side effects, not allergies.
If you’re unsure, don’t guess. See an allergist. A detailed history, skin test, and sometimes an oral challenge can give you a clear answer.
What to Do If You Think You’re Allergic
If you’ve been told you’re allergic to a drug:
- Check your symptoms. Was it a rash? Was it after a virus? Did it happen once, years ago?
- Don’t avoid the drug unless you’ve been tested. Many people unnecessarily avoid life-saving or best-choice medications.
- Ask your doctor about referral to an allergist. Testing is safe, fast, and often covered by insurance.
- If you’ve had a severe reaction (anaphylaxis, SJS, or breathing trouble), get tested before trying the drug again.
- Update your medical records. If testing shows you’re not allergic, make sure your GP and pharmacy know.
One patient in Sydney, 52, was told she was allergic to penicillin after a rash at age 8. She spent 30 years on stronger antibiotics, got three C. diff infections, and paid over $15,000 extra in medical bills. After testing, she was cleared. She now takes penicillin safely-and her infections are gone.
What’s Changing in Drug Allergy Care
Things are improving. Hospitals are starting pharmacist-led screening programs. Telehealth penicillin allergy clinics now cut wait times from 60 days to under two weeks. Genetic testing for HLA-B*1502 is becoming routine before prescribing carbamazepine in high-risk groups.
Next up? Point-of-care genetic tests for other high-risk drugs like allopurinol and abacavir. Within five years, your doctor might check your DNA before prescribing-not just to avoid reactions, but to choose the best drug for your body.
The message is clear: don’t live with a label you never tested. Drug allergies are real-but many are mislabeled. And getting the truth could save your life-or at least, your wallet and your health.
Can you outgrow a drug allergy?
Yes, especially with penicillin. Studies show 80% of people labeled allergic as children lose their allergy after 10 years without exposure. The immune system forgets. But you shouldn’t assume you’re no longer allergic-you need testing to be sure.
Is a rash always a sign of drug allergy?
No. Many rashes that appear after taking a drug are caused by viruses, not the medication. In fact, up to 20% of children who get a rash after antibiotics have a concurrent viral infection. A true allergic rash is often itchy, raised, and spreads quickly. Delayed rashes (after 7+ days) are more likely to be T-cell mediated and need careful evaluation.
Can you be allergic to all NSAIDs?
Not necessarily. People with aspirin-exacerbated respiratory disease must avoid all non-selective NSAIDs (like ibuprofen and naproxen). But they can often tolerate COX-2 inhibitors like celecoxib. If you’re unsure, an allergist can do a controlled challenge to see which drugs you can safely take.
Why is penicillin allergy testing so accurate?
Because the test uses the actual drug components. Skin testing with penicillin derivatives (like Pre-Pen) detects IgE antibodies specific to the drug. When combined with a supervised oral amoxicillin challenge, the test is 97-99% accurate at ruling out true allergy. It’s one of the most reliable tests in all of allergy medicine.
Do I need to avoid all antibiotics if I’m allergic to one?
No. Antibiotics are grouped by chemical structure. Being allergic to penicillin doesn’t mean you’re allergic to all antibiotics. Cephalosporins, tetracyclines, and azithromycin are unrelated and usually safe. Cross-reactivity between penicillins and cephalosporins is only 1-3%. Always ask your doctor or allergist which alternatives are safe for you.
Can I be tested for allergies to chemotherapy drugs?
Yes. For drugs like paclitaxel or cetuximab, allergists use desensitization protocols-gradually increasing doses under medical supervision-to safely administer the drug even after a previous reaction. Testing isn’t always possible, but desensitization works in 80-90% of cases. It’s a standard part of cancer care in major hospitals.

Melissa Stansbury
March 17, 2026 AT 22:16I was told I was allergic to penicillin at 7 after a rash-turns out it was just heat rash from a fever. I avoided it for 25 years until I finally got tested. Turned out I’m fine. Now I take amoxicillin like it’s candy. My last UTI? Gone in 48 hours. Saved me $12k in hospital bills and three rounds of C. diff. Why didn’t anyone tell me this sooner?
My doctor didn’t even mention testing. Like, we just assume you’re allergic forever? That’s insane.
cara s
March 18, 2026 AT 00:00It is, quite frankly, astonishing, and frankly, almost criminal, that the medical establishment has allowed this outdated, fear-based, and statistically unsound paradigm to persist for so long-wherein individuals are permanently labeled as "allergic" based on anecdotal, unverified, and often misattributed childhood events-when modern diagnostic tools, such as skin prick testing and supervised oral challenges, exist with a reliability of 97–99%.
And yet, we continue to prescribe broader-spectrum antibiotics, which not only cost more, but also accelerate antimicrobial resistance, increase hospital stays, and contribute to the rise of deadly superinfections like C. diff. This isn’t just negligence-it’s systemic inertia cloaked in tradition. We need mandatory allergist referrals for any penicillin label, especially if it predates adolescence. The data is clear. The cost is staggering. The moral imperative? Unignorable.
Amadi Kenneth
March 19, 2026 AT 05:37Wait… so you’re telling me Big Pharma and the FDA are hiding something? Why do they WANT people to avoid penicillin? Because vancomycin? Ceftriaxone? Those are EXPENSIVE! And they’re not natural! They’re lab-made! And who profits? Hospitals! Insurance companies! Drug manufacturers! They don’t want you to get tested-they want you stuck on the expensive stuff!
And what about the HLA-B*1502 thing? Why is it only tested in Asians? What about Africans? Latinos? They get SJS too! It’s a cover-up! They’re profiling people based on ethnicity to sell more drugs! I’ve got cousins in Nigeria who got rashes from carbamazepine-they were never warned! This is genocide by prescription!
Shameer Ahammad
March 20, 2026 AT 12:15Let me be perfectly clear: if you have ever been told you have a "drug allergy," without objective testing, you are, in fact, a statistical liability to your own health-and to the broader public health infrastructure. The notion that a single childhood rash, occurring during a viral illness, constitutes a lifelong contraindication to a first-line antibiotic is not merely archaic-it is dangerously irrational.
Furthermore, the failure of primary care providers to refer patients for allergist evaluation represents a catastrophic breakdown in clinical diligence. The cost of mislabeling is not anecdotal-it is quantifiable: prolonged hospitalization, increased antibiotic resistance, and avoidable mortality. We must institutionalize pre-prescription allergy verification. No more assumptions. No more legacy labels. Evidence-or nothing.
Srividhya Srinivasan
March 20, 2026 AT 15:47Oh my GOD, I’ve been screaming this from the rooftops since 2018!! I got a rash on amoxicillin when I was 5-"allergy" stamped on my chart. Fast forward 30 years-I had a UTI, got prescribed cipro because "penicillin allergy"-C. diff hit me like a freight train. Three hospitalizations. Lost my job. My insurance raised my rates. I cried in the pharmacy aisle when I found out I could’ve taken penicillin the whole time!!
And now they want to test for genetic markers? That’s great-but what about the 80% of people who never even heard of an allergist? We need public campaigns. Billboards. TikTok videos. This isn’t niche-it’s a MASSIVE public health crisis, and nobody’s talking about it!!
Also-why is it always "women’s health" that gets attention? My brother died from a mislabeled allergy. Nobody cared. #DrugAllergyAwareness
Stephen Habegger
March 21, 2026 AT 18:40This is the most important thing I’ve read all year. If you think you’re allergic to penicillin-get tested. It’s quick, cheap, and could save your life. Seriously. Do it.
Justin Archuletta
March 23, 2026 AT 13:25I got tested last year after reading this. Turned out I wasn’t allergic. Took amoxicillin for a sinus infection. No problem. Felt like I got my health back. Thanks for the info!
P.S. My doctor didn’t even know about the testing. Had to push for it. Wild.
Kendrick Heyward
March 25, 2026 AT 13:12They’re lying to you. They don’t want you to know you can get tested. Why? Because if you find out you’re NOT allergic, you’ll stop taking their expensive antibiotics. And they’ll lose BILLIONS.
I read this article and then looked up the FDA’s funding sources. Guess what? They’re funded by the same companies that make vancomycin.
They’re gaslighting us. I’m not taking another drug until I get a lawyer. 😔
lawanna major
March 27, 2026 AT 04:01There’s a deeper truth here: we treat medical labels as identity, not as provisional data. We don’t question a penicillin allergy like we’d question a childhood diagnosis of "asthma" or "ADHD"-we cling to it. Why? Because uncertainty is terrifying. It’s easier to say "I’m allergic" than to admit we don’t know.
But medicine isn’t about certainty-it’s about evidence. And evidence shows that 90% of us were mislabeled. That’s not a coincidence. It’s a failure of systems designed to protect us, but instead, they’ve imprisoned us in outdated fear.
Maybe the real allergy isn’t to penicillin-it’s to curiosity. To asking, "What if I’m wrong?"
Let’s get curious.
Ayan Khan
March 28, 2026 AT 03:33As someone from India, I’ve seen firsthand how drug allergies are misunderstood. Many people here avoid antibiotics because of a rash from childhood, not knowing that a viral infection was the real culprit. We need more awareness campaigns-not just in the U.S., but globally.
And the genetic testing point? It’s brilliant. HLA-B*1502 is common in South Asia too. Why aren’t we screening before prescribing carbamazepine here? It’s not just a Western issue-it’s a human issue.
I’m sharing this with my family. We all need to question our labels. Knowledge is power.
Kal Lambert
March 28, 2026 AT 21:06Testing works. I got mine done. Wasn’t allergic. Took penicillin. Fine. My doctor didn’t even know how to order the test. Had to Google it. Go to an allergist. Took 20 minutes. Worth it.
Stop assuming. Start testing.
Nilesh Khedekar
March 30, 2026 AT 01:14so uhh like i got the penicillin label too but then i took it once on purpose just to see and i was fine?? like i dont even know why we do this anymore??
my mom said i was allergic when i was 4 and now im 32 and i just took amox and nothin happened??
Robin Hall
March 30, 2026 AT 12:17The systemic failure to address mislabeled drug allergies constitutes a breach of the standard of care. The persistence of this practice, despite overwhelming evidence to the contrary, demonstrates a profound dereliction of duty by medical institutions, regulatory bodies, and educational establishments. The economic, clinical, and epidemiological consequences are not merely unintended-they are predictable, preventable, and therefore, morally indefensible.
Until mandatory re-evaluation protocols are implemented for all drug allergy labels established before age 18, this issue remains an active, ongoing public health emergency.
Melissa Stansbury
April 1, 2026 AT 10:52You’re telling me your doctor didn’t even suggest testing? That’s the problem right there. I had to beg mine. They said, "It’s not worth it." I said, "I’ve had three C. diff infections." Then they called the allergist. I’m so mad I wasted 25 years.
Why aren’t they doing this proactively? Why is it on us to fight for our own health?