
Why Renal Ultrasound Is the First Step for Kidney Problems
If you’re being checked for kidney pain, frequent urinary tract infections, or high blood pressure, your doctor might start with a simple ultrasound. That’s because renal ultrasound is the safest, fastest, and most widely used way to check for kidney obstruction and measure kidney size-without radiation, needles, or contrast dye. It’s not fancy, but it works. In emergency rooms, hospitals, and even some GP clinics across Australia and the U.S., this test is the go-to for spotting blockages early.
Imagine your kidneys as water filters. When urine can’t flow out properly-maybe because of a stone, scar tissue, or a narrowed tube-the pressure builds up. That’s called hydronephrosis. The kidney swells, the cortex thins, and if left unchecked, it can damage the organ permanently. Renal ultrasound picks up these changes before you even feel serious symptoms. It doesn’t just show if something’s wrong-it tells you how bad it is.
What Does a Renal Ultrasound Actually Show?
During the scan, a technician moves a small handheld device over your back or abdomen. It sends out sound waves that bounce off your kidneys and create real-time images on a screen. What they’re looking for isn’t just shape-it’s size, structure, and flow.
- Kidney length: Normal adult kidneys are 9 to 13 centimeters long. Anything shorter than 9 cm might mean chronic damage or shrinkage.
- Cortical thickness: The outer layer of the kidney should be at least 1 cm thick. If it’s thinner, that’s a red flag for long-term scarring or pressure damage.
- Renal pelvis diameter: The central part of the kidney where urine collects. A measurement over 7 mm in adults suggests fluid buildup-hydronephrosis.
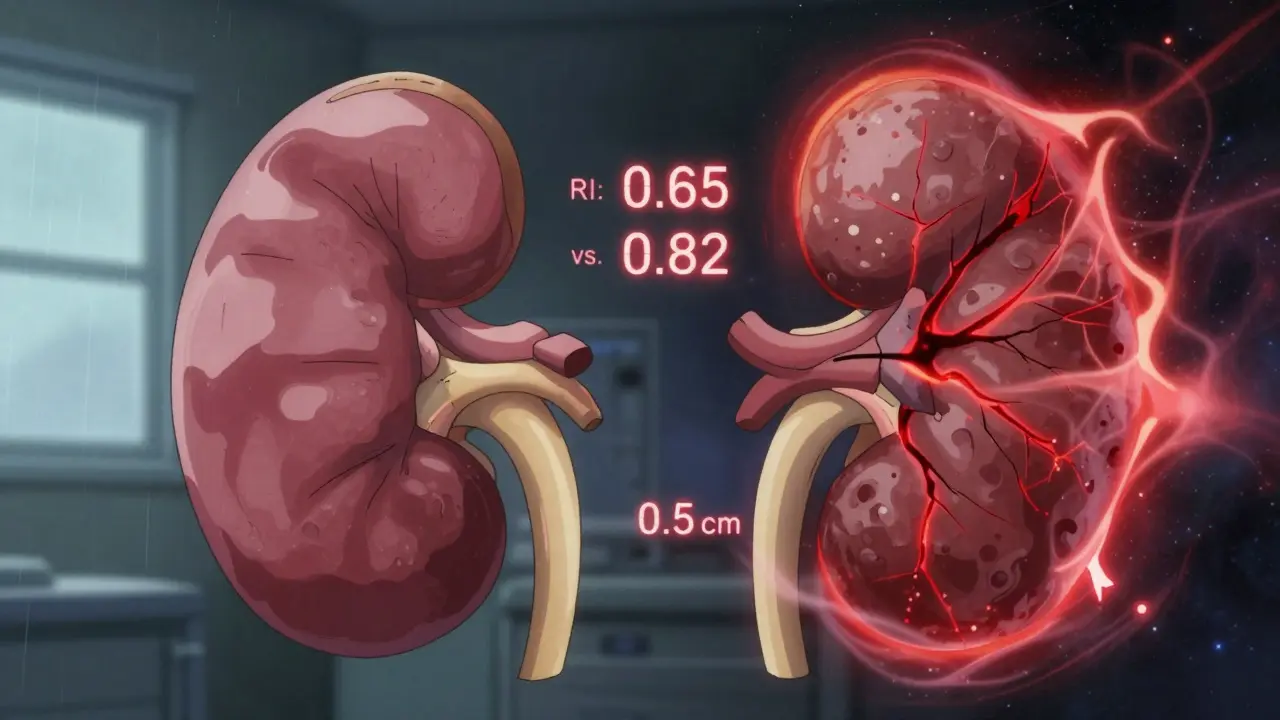
- Resistive index (RI): This isn’t visible on the picture, but it’s calculated from Doppler ultrasound. It measures how easily blood flows through the kidney’s tiny arteries. An RI above 0.70 strongly suggests obstruction. Studies show it’s 87% accurate at catching blockages.
These numbers matter. A kidney that’s 11 cm long with a 1.2 cm cortex and an RI of 0.65? Probably fine. A kidney that’s 7 cm long, cortex at 0.5 cm, and RI at 0.82? That’s a kidney under serious stress-and needs urgent attention.
How Ultrasound Finds Obstruction-And Where It Falls Short
Ultrasound excels at showing the effects of blockage: swelling, stretched tubes, thickened walls. But it doesn’t always show the cause. A stone might be invisible if it’s small or hidden behind bowel gas. That’s why some people end up needing a CT scan later.
Here’s the reality: ultrasound finds about 80% of kidney stones larger than 3 mm. Smaller ones? Often missed. CT scans catch stones as small as 1-2 mm. But CT gives you radiation-about 10 millisieverts per scan. That’s the same as three years of natural background radiation. For someone with recurring stones, repeated CTs add up. Ultrasound avoids that.
It’s also better for pregnant women, kids, and people with kidney failure who can’t handle contrast dye. In fact, in pediatric cases, ultrasound is the gold standard. A child with suspected ureteropelvic junction (UPJ) obstruction? Ultrasound is the first-and often only-test needed.
But it has limits. In patients with high BMI (over 35), sound waves can’t penetrate well. The images get blurry. That’s when doctors turn to MRI or CT, even with the risks. Also, ultrasound can’t measure how fast urine drains from the kidney. That requires a nuclear scan or advanced CT algorithms. So while ultrasound tells you there’s a backup, it doesn’t always tell you how fast it’s filling.
Doppler and Elastography: The New Tools Making Ultrasound Smarter
Ultrasound isn’t stuck in the 1980s. Two big advances are changing how we use it: Doppler and shear-wave elastography.
Doppler ultrasound measures blood flow speed. In a healthy kidney, blood moves easily. In an obstructed one, the arteries stiffen. That’s where the resistive index comes in. It’s not just a number-it’s a warning sign. When RI hits 0.70 or higher, it’s like a red light flashing: “This kidney is fighting pressure.”
Shear-wave elastography is even newer. It measures how stiff the kidney tissue is. Think of it like poking a water balloon. A normal kidney is soft and gives a little. An obstructed one becomes stiff-like a rock. Studies show stiffness increases linearly with pressure. That means, in the future, we might not just see swelling-we might measure how much pressure is building inside the kidney. That’s huge for tracking treatment progress.
Some hospitals are now using AI to auto-calculate hydronephrosis grades. Instead of a radiologist eyeballing dilation, software analyzes the image and gives a score. Early results are promising. One 2023 trial at Mayo Clinic showed AI matched expert readings 92% of the time.
Who Performs the Scan-and Why Skill Matters
Not all ultrasounds are created equal. A nurse in the ER doing a quick check for stones? Different from a certified sonographer doing a full renal evaluation.
Studies show up to 20% variation in kidney size measurements between inexperienced and expert operators. One person might measure a kidney at 10 cm. Another, using the same machine, gets 11.5 cm. That’s not a machine error-it’s technique. The difference? Knowing exactly where to place the probe, how to angle it, and which landmarks to follow.
The American Institute of Ultrasound in Medicine (AIUM) says you need at least 40 supervised scans to be certified. And even then, mastery takes more. Radiology residents report needing around 50 exams before they feel confident reading resistive index values. That’s why some hospitals now require a second opinion for borderline cases.
Point-of-care ultrasound-done bedside by emergency doctors-is growing fast. In major U.S. hospitals, 75% of emergency departments now use it for suspected kidney stones. It cuts diagnosis time by nearly 45 minutes. But it’s not a replacement for a full diagnostic scan. It’s a triage tool: “Is this urgent? Do we need a CT now-or can we wait?”
How Often Should You Get One?
Most people only need one renal ultrasound if they’re being checked for a single episode of pain or infection. But for chronic conditions, it becomes a monitoring tool.
Take someone with a history of ureteropelvic junction (UPJ) obstruction after surgery. Instead of repeated CTs every few months, their urologist might order a quick ultrasound every 4-6 weeks. It’s safe, cheap, and gives a clear picture of whether the repair is holding. One urologist in Sydney told me: “I’d rather see a blurry ultrasound every week than a sharp CT every month.”
For people with polycystic kidney disease, hypertension, or recurrent UTIs, annual ultrasounds are common. It’s not about finding stones-it’s about watching for slow shrinkage or new blockages. Kidneys don’t scream when they’re failing. They just get smaller, thinner, and stiffer. Ultrasound catches that quietly.
What Comes After the Ultrasound?
If the ultrasound shows mild hydronephrosis and a normal RI? You might just be told to drink more water and come back in a few weeks.
If it shows severe dilation, thin cortex, and high RI? The next step is usually a CT urogram or MR urogram to find the exact location of the blockage. That’s when you might see a urologist for a stent, surgery, or other intervention.
But here’s the key: ultrasound often prevents the need for more invasive tests. In one 2022 study, 40% of patients referred for CT after kidney pain had normal ultrasounds. That meant they avoided radiation, contrast, and unnecessary cost.
Ultrasound doesn’t answer every question. But it answers the most important one: “Is something wrong with the kidney’s structure-and is it getting worse?”
What to Expect During the Test
No fasting. No injections. No radiation. Just lie on your back or side while a gel is applied to your skin. The probe glides over your flank and lower back. You might feel slight pressure, but no pain.
The whole thing takes 15 to 30 minutes. You can drive home right after. Results are often available the same day, especially in hospitals. In some clinics, your doctor gets the report within hours.
There’s one small prep tip: drink a glass of water an hour before. A full bladder helps push bowel gas out of the way and gives a clearer view of the lower kidneys and ureters.
Why This Test Won’t Be Replaced Anytime Soon
There are fancy new imaging tools. AI. Super-resolution ultrasound. 3D mapping. But none of them match renal ultrasound’s balance of safety, speed, cost, and accessibility.
It costs $200-$500 in the U.S. A CT scan? $1,200-$2,500. An MRI? $1,500-$3,000. Ultrasound machines are portable. You can carry one in a backpack. In rural Australia, mobile ultrasound vans now visit remote clinics. That’s life-changing for people who can’t travel to big hospitals.
And it’s not going anywhere. The American Urological Association predicts renal ultrasound will remain first-line through 2030. Even with AI and new tech, the core strength stays: it shows you the kidney’s structure without hurting you. That’s why it’s used in over 12 million U.S. patients every year-and why it’s the standard in Australia, the UK, and Canada too.
Final Thought: It’s Not About the Machine. It’s About the Message.
A renal ultrasound doesn’t just give you a picture. It gives you a story: Is the kidney swollen? Is it shrinking? Is the blood flow restricted? Is pressure building? That story guides treatment. It tells you whether to wait, to operate, to monitor, or to refer.
It’s not glamorous. But in medicine, the best tools aren’t always the flashiest. Sometimes, they’re the quiet ones that keep working-year after year-without asking for a credit card.
Can a renal ultrasound detect kidney stones?
Yes, but not always. Ultrasound can detect most kidney stones larger than 3 mm, especially if they’re in the kidney or upper ureter. Smaller stones, or those hidden behind bowel gas, may not show up. CT scans are better for finding tiny stones, but ultrasound is preferred for initial screening because it avoids radiation and contrast.
What is hydronephrosis, and how does ultrasound detect it?
Hydronephrosis is swelling of the kidney caused by urine backup, usually due to a blockage. Ultrasound detects it by measuring the anteroposterior diameter of the renal pelvis. If it’s over 7 mm in adults, it’s considered abnormal. The scan also shows dilated tubes (calyces) and sometimes thinning of the kidney’s outer layer, which signals long-term pressure damage.
Is a high resistive index always a sign of obstruction?
Not always, but it’s a strong indicator. An RI above 0.70 has 87% sensitivity for obstruction. However, other conditions like kidney infection, chronic disease, or severe dehydration can also raise the RI. That’s why doctors look at it along with kidney size, cortical thickness, and clinical symptoms-not in isolation.
Can obesity affect the accuracy of a renal ultrasound?
Yes. In patients with a BMI over 35, sound waves have trouble penetrating deep tissue. This leads to blurry images and unreliable measurements. In these cases, doctors often switch to CT or MRI, even though they involve radiation or higher cost. Portable ultrasound devices with better penetration are helping, but obesity remains a major limitation.
How often should someone with kidney issues get a renal ultrasound?
It depends. For a one-time issue like a kidney stone, one scan is usually enough. For chronic conditions like UPJ obstruction, polycystic kidney disease, or post-surgery monitoring, scans every 3 to 6 months are common. The goal is to track changes in size, thickness, and blood flow over time-without exposing the patient to repeated radiation.




Jason Xin
January 31, 2026 AT 21:08Bobbi Van Riet
February 1, 2026 AT 23:02Holly Robin
February 3, 2026 AT 15:57Shubham Dixit
February 4, 2026 AT 12:41Blair Kelly
February 4, 2026 AT 21:39Rohit Kumar
February 5, 2026 AT 03:25Lily Steele
February 5, 2026 AT 16:10Gaurav Meena
February 6, 2026 AT 15:29Amy Insalaco
February 7, 2026 AT 08:22